- New principles of best practice in clinical audit (HQIP, Radcliffe Publishing, 2011)
- Quality Improvement Made Simple. The Health Foundation. Website link. https://www.health.org.uk/sites/default/files/QualityImprovementMadeSimple.pdf
- The New Economics for Industry, Government and Education (1994), Dr W Edwards Deming
- The Meaning of Quality and the Juran Trilogy. Q Community Article. Updated March 2025. https://q.health.org.uk/evidence-and-insights/opinion-pieces/the-meaning-of-quality-and-the-juran-trilogy
- Royal College of Physicians National Audit Programme. Website link. https://www.rcp.ac.uk/improving-care/national-clinical-audits/
The challenge of modern-day clinical audit for clinicians
It's close to midnight
It’s close to midnight and something evil is lurking in the dark. No, this blog is not a homage to Michael Jackson’s ‘Thriller’ song. Rather, it is setting the scene for a resident doctor who has just finished her late 3pm-11pm shift in the medical assessment unit . She is now sitting quietly in a back-room office trying to finish the last batch of data collection for her clinical audit. The prospect of going through another pile of medical notes is daunting. The day shift was busy - tiring to be honest - and there was little chance to do this ‘audit stuff’ during the working day. She knows she will rotate soon to her new gastroenterology department in a few days.
She reflects on how she first got involved in the clinical audit. It all felt a bit random and unplanned. The day-time medical consultant was frustrated at the lack of clinical documentation in the medical clerking booklet. He suggested to do an audit to help her e-portfolio. “Why don’t you find out how bad it is…” She had quickly found some clinical standards on Google to benchmark the audit against. Further thoughts crossed her mind. Perhaps it would have been better if she registered the audit? Who was going to review this audit when she moves on? Is someone doing a similar audit elsewhere in the hospital? Does this audit count as QI? Was the audit enough to evidence her commitment to quality and safety? It all felt disjointed. She wished she had some guidance on how to do audits and a clinical mentor to support her.
Maybe the next F2 doctor can do an audit intervention bit? Knowing that she had little chance of doing the ‘interventions’ herself or complete a second audit cycle. She thought about how long the audit data collection had taken her and wondered whether some of the questions in the audit were even relevant. She sighed and prepared herself for the next set of notes.
This fictional account highlights some of the issues that can arise when clinical audit is not supported properly. Resident doctors and other clinicians often cite a lack of understanding of clinical audit processes, clinical work pressure challenges, time constraints to collect data, and lack of mentorship/organisation support. All of which can contribute to clinicians feeling stressed and burnt out.
In the rest of this blog, I will explore these areas further and suggest potential strategies to resolve them.
The Clinical Audit and Quality Improvement (QI) - dancing partners?
The interplay between clinical audit and QI remains a grey area to many clinicians. They have been described as ‘dancing partners’. To explore their relationship further, let us start with a definition of each.
Both definitions are reasonable but they highlight potential areas of overlap. Audit can be described as a tool under the big umbrella of Quality Improvement. Conversely (and sometimes confusingly), modern definitions of a clinical audit cycle have QI methodology within it.
The figure below attempts to illustrate this. In clinical audit, once we have defined the audit criteria and benchmarking standard, we proceed to collecting data and then compare with the standards to identify the quality gap. It is at the implementation of change of clinical audit, we begin to think differently.
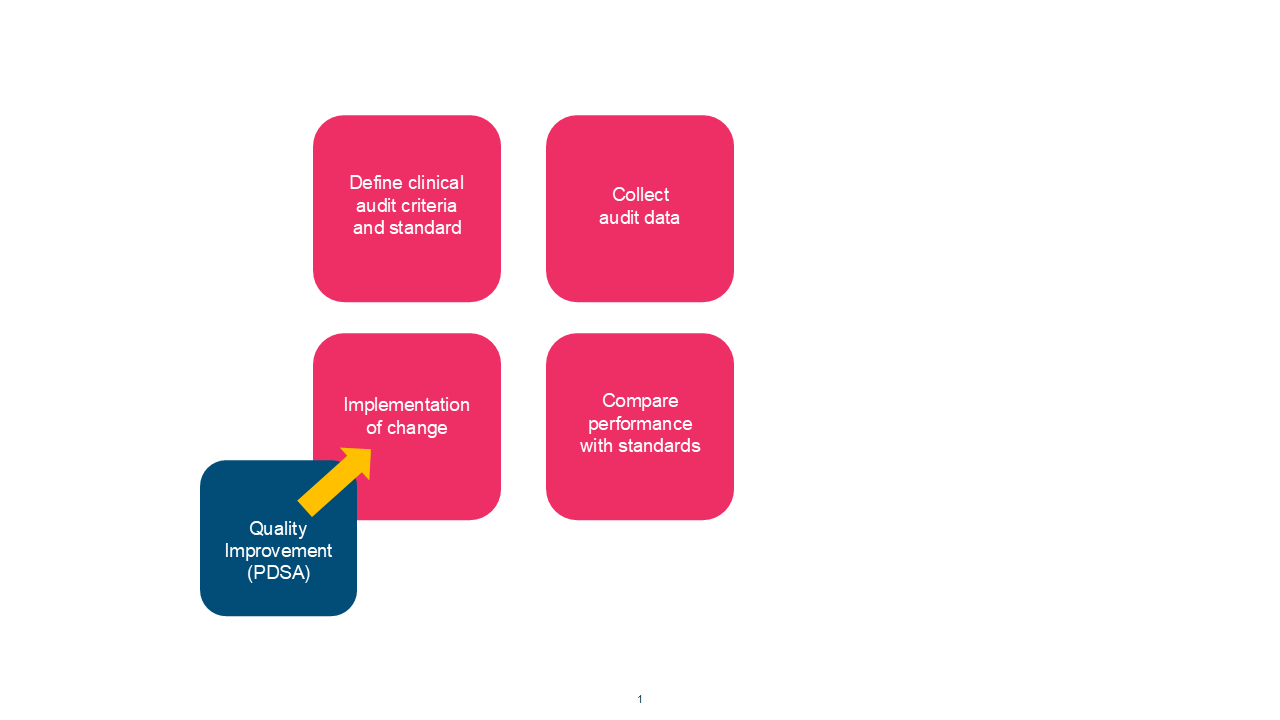
In traditional audit, sometimes a single intervention is considered before starting audit cycle 2. But there are problems with this approach… How will we know what is the right intervention? Dr Edward Deming3 talks about the theory of improvement and suggests a deeper understanding of a problem is needed. He calls it the “System of Profound knowledge”. To implement effective change, we need a full appreciation of the system and the knowledge that lies within. We need to explore the psychology of the teams that work in that system. Most importantly, we need to understand the variation that exists in the current data. Without this we are likely to do the wrong thing.
The blue box in the figure shows where we should use QI methodology, often through iterative learning through plan, do, study, act (PDSA) cycles.
How do acute hospitals trusts integrate QI and clinical audit as part of a Quality Management System?
We often refer to Juran’s trilogy when thinking about a framework for a Quality Management System (QMS). The three QMS components are quality planning, quality improvement and quality control. All three components are needed for safe and effective outcomes for our patients. Clinical audit is considered a tool for quality control.
Given the close interplay between clinical audit and QI, it would be a reasonable to think that QI and clinical audit departments work closely together. This is not necessarily true. Quality improvement teams (often housed within Strategy and Improvement departments) are relatively new in the NHS, whereas clinical audit teams have been around for decades. Staff can be invested in their respective approaches; to either traditional clinical audit methods, or quality improvement. These ‘tribal’ teams tend to highlight their differences in approach rather than their commonality, leading to misunderstanding, power dynamics with competing funding streams for workforce. None of this helps clinicians to do good effective clinical audit and hampers their ability to use improvement methodology within clinical audits.
As clinicians, we should be focusing on the first three audit categories on the list above. In our fictional story, the clinical audit was proposed at a whim, stemming from the initial frustration of the consultant during a clinical ward round. I would probably classify this as a ‘non-priority local clinical audit’. Performing non-priority local audits as a resident doctor may not impact significantly on quality outcomes for patients and can often be left abandoned after the first cycle. The auditing doctor has likely moved departments and the sponsor may have lost interest to continue.
One of the key roles of a clinical audit lead is to coordinate the audit activity of their department and ensure alignment to the departmental strategy and clinical risks. They are also the support link for national/core audits. When clinical audit is done well, it always forms part of a QMS.
Final thoughts
I hope this blog has helped us to reflect on where the opportunities and challenges are for clinical audit in acute hospitals. The NHS continues to work with an often stressed workforce and an ever-smaller financial envelope. We must ensure that our clinicians undertake clinical audit within a clearly defined quality management system. Only then can we ensure effective clinical outcomes for our patients.
Secondly, the ‘dancing partner’ relationship between clinical audit and QI needs to be better understood and explained. Organisations should find ways to integrate the work/processes between QI teams and clinical audit departments. In my view, they should all be one team!
To finish with, we have a responsibility to ensure that large national audit datasets collected by our clinicians across the country are owned by the local teams who are collecting the data. Clinicians are less interested in published yearly national datasets. They want timely access to their local benchmarked departmental audit data all year round, so that they can get on with the important business of improving. Isn’t that why we are all here?



